DPR
Dissociated Pain Release
A self-help technique developed by a trauma survivor

Anne MacMillan, MLA
Survivor, Consultant, Coach
Master's Clinical Psychology - Harvard University
Dissociated Pain Release
Self-Help Trauma Support
Dissociated Pain Release
Dissociated Pain Release (DPR) is a self-help technique that allows users to release emotional pain from trauma without re-experiencing it. It is based on the idea that emotional pain is stored in the mind, body, and nervous system and that the stored pain causes distress and discomfort in the present, whether the trauma was a recent event or something that happened many years ago.
There is no need for a DPR user to know where any emotional pain came from. All a user needs to know is that they are currently experiencing unwanted emotional pain and that they would like to release that pain and feel better -- quickly.
Most importantly, in DPR, emotional pains are released while the user is dissociated from them -- allowing the user to process any trauma or distress without being forced to relive the original traumatic experience.
Examples of emotional pain that can be released from the body and nervous system through DPR include rage, anger, shame, sadness, guilt, grief, loneliness, abandonment, anxiety, and fear.
Likewise, DRP allows users to release any stored sensations associated with physical pain or forms of bodily discomfort that happened in the past. DPR users can release sensations of nausea, dizziness, cold, being drugged, etc. Again, all these sensations are released without the DRP user re-experiencing the original potency of any traumatic event. Often DPR users release pain without even knowing what the original traumatic event may have been.
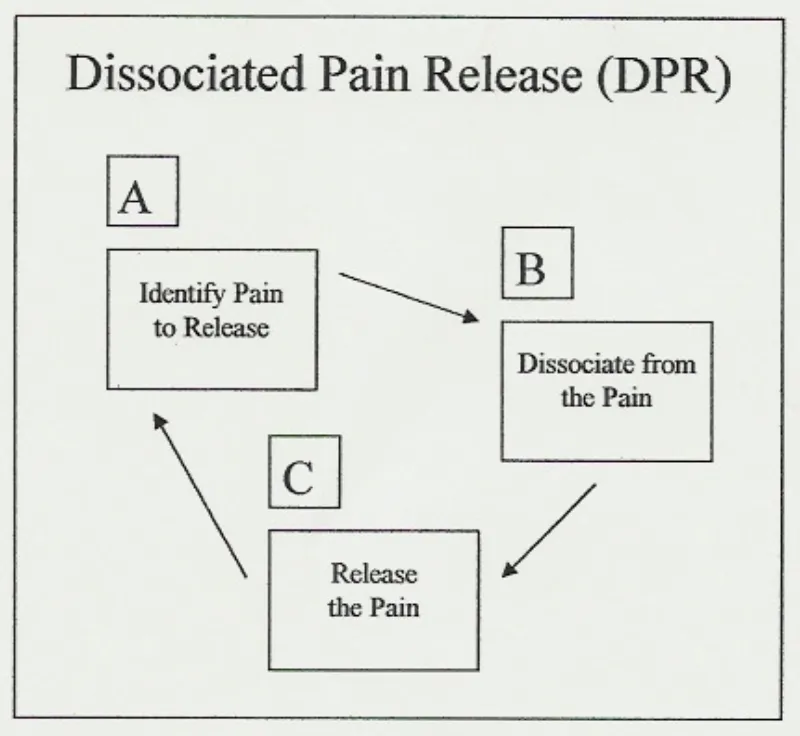
DPR has three cyclical steps: (A) identify pain to release, (B) dissociate from the pain, and (C) release the pain. Once understood, DPR is a simple, repetitive process that applies in many self-help situations. Any user employing DPR expects to complete its A-B-C cycle several times in any one self-help session. It is understood that there may be several painful emotions, different forms of physical pain and other negative bodily sensations that require release, making time and repetition necessary.
IMPORTANT
* DPR is not trauma therapy.
Anne is not a therapist and does not support individuals through trauma therapy. Anne teaches a self-help technique that individuals can apply to many situations in their everyday lives and that they have a right to use to manage any experiences they choose, traumatic or not. It is always recommended that trauma survivors hire a licensed trauma therapists whenever possible. Call 911 in any emergency.
Feeling Suicidal?
Find a Helpline

Anne MacMillan, MLA
Survivor, Consultant, Coach, Educator
Master's Clinical Psychology, Harvard Univerisity
IMPORTANT
* DPR is not trauma therapy.
Anne is not a therapist and does not support individuals through trauma therapy. Anne teaches a self-help technique that individuals can apply to many situations in their everyday lives and that they have a right to use to manage any experiences they choose, traumatic or not.
It is always recommended that trauma survivors hire a licensed trauma therapists whenever possible. Call 911 in any emergency.
Feeling Suicidal?
Find a Helpline:
https://findahelpline.com/
About Me
Like many others, I grew up in a household that didn't offer me the basic protections all children need. I experienced extreme trauma as a very young child and, unfortunately, that trauma continued into my adolescence and adulthood.
I survived adolescence emotionally by focusing on studying contemporary dance, helping me process my emotions and increase my body awareness. As a young adult in my twenties, I was exposed to relaxation and meditation techniques and the idea that healing that comes naturally when we move our eyes as we dream.
In my mid-twenties, memories of traumatic events that had happened during my early childhood began to return to my consciousness. I knew about EMDR (Eye-Movement Desensitization and Reprocessing) therapy for trauma, but wasn't in a situation that allowed me consistent access to a trauma therapist.
So, I began working through my traumatic memories on my own, combining what I'd learned about the emotions I felt in my body through dancing with relaxation and visualization techniques. I added what I decided to call REM Simulation -- or Rapid Eye Movement Simulation. REM sleep is the deep dreaming sleep in which humans naturally process emotions.
The result was a self-help technique that made it possible for me to work through the terrible emotions associated with traumatic events that had occurred in my past and regain the sense of emotional stability I needed -- all without having an opportunity to get the therapeutic support I needed.
Dissociated Pain Release
I dubbed my self-help technique DPR, or Dissociated Pain Release, and decided that I didn't want it to ever become something that anyone with an advanced degree and a lot of privilege could tell people they weren't qualified to perform at home on their own.
Therapy is wonderful and everyone who has access to a therapist should take advantage of that privilege. But recovery strategies should be available to anyone anywhere. That's what DPR is about for me.
From my perspective, DPR is nothing more than a collection of practical ideas put together in one package to help all of us get through the difficult emotions humans feel. It's valuable because it works and it uses human's natural REM (Rapid Eye Movement) sleep processing methods.

My Newest Blog Posts

How Intimacy Forms Along the Non-Autistic Pathway
Series V, Article 2: How Intimacy Forms Along the Non-Autistic Pathway
The non-autistic developmental pathway has been described across this series as an oscillation: a continuous back-and-forth between going out into the world and curving back to integrate what came back, between the forward movement of assimilation and the integrating movement of accommodation. That oscillation drives trust, autonomy, identity formation, and every other developmental achievement the pathway is oriented toward. It also drives intimacy. And understanding how it does requires understanding what the oscillation is actually built from at its core: the continuous, embodied, largely automatic reception of social and emotional information from the people around it (Craig, 2009; Critchley et al., 2004; Decety & Jackson, 2004; Gallese, 2009; Niedenthal, 2007).
Body empathy, MacMillan's term for this reception, is not simply the capacity to notice that another person is having an experience. It is the capacity to register that experience in one's own body, in real time and below the level of conscious awareness, in a way that makes the distinction between one's own emotional state and another person's genuinely porous at the edges (Craig, 2009; Critchley et al., 2004; Lamm et al., 2007; Singer et al., 2004). That porousness is what makes the non-autistic nervous system so well suited to the intimacy process. And it is also what makes the specific vulnerabilities of the non-autistic pathway in intimacy so particular.
The Mechanism of Disclosure
The research on intimacy as an interpersonal process, developed through the work of Reis and Shaver and extended by Laurenceau and colleagues, establishes intimacy as built from three movements: one person discloses something genuine about themselves, the other discloses in return, and the first person feels genuinely received by the response (Laurenceau et al., 1998; Reis & Shaver, 1988). What makes this a process of intimacy rather than simply an exchange of information is the third movement: the experience of being received. Not agreed with, not evaluated, not advised, but genuinely received. The sense that what was offered landed in the other person as something that mattered, was taken seriously, and was held with care (Laurenceau et al., 1998; Reis & Gable, 2015; Reis et al., 2017).
Social penetration theory, developed by Altman and Taylor, adds another dimension: intimacy is not only about the quality of disclosure but its depth (Altman & Taylor, 1973). Relationships move from surface-level exchange toward genuine closeness as the disclosures become progressively more revealing, more personal, and more vulnerable. This is not a linear process and it is not a deliberate strategy. It is what happens when two people trust each other enough to offer more of themselves, and when that offering is consistently met with the genuine reception that makes the next offering feel safe (Altman & Taylor, 1973; Laurenceau et al., 1998).
For the non-autistic nervous system, this process is not entirely voluntary. Body empathy means that the emotional states of the people nearby arrive continuously and without effort. Many non-autistic people in a conversation with someone they are close to ar already, before any deliberate self-disclosure, registering something of that person's experience in their own body. They are orienting toward the other, feeling for the shape of what is present between them, and adjusting in real time. The intimacy mechanism is not something they turn on. It is something that runs (Craig, 2009; Decety & Jackson, 2004; Gallese, 2009; Niedenthal, 2007).
What the Non-Autistic Person Is Actually Offering
When a non-autistic person shares something personal, something of their inner experience, their self-reflection, their uncertainty, their joy, their difficulty, they are not primarily providing information. They are extending an intimacy bid (Laurenceau et al., 1998; Reis & Shaver, 1988). The disclosure is an offering of the self, a gesture toward genuine knowing, a way of saying: here is something of what it is like to be me. The implicit question in the offering is not what do you think about this, but do you receive me? (Reis & Gable, 2015; Reis et al., 2017).
The reception they need in response is specific. It is not a solution to the problem described. It is not an evaluation of whether their experience is reasonable. It is the felt sense that what they offered landed: that the other person was genuinely present to what was shared, was moved by it in some way, and held it with the care the disclosure invited (Laurenceau et al., 1998; Reis & Gable, 2015; Reis et al., 2017). That felt sense, when it arrives, is itself the intimacy. The closer one is known, the more the disclosures that are met with genuine reception become the substance of the relationship itself: the accumulated experience of having been genuinely seen by this particular person, in these particular moments, over time (Altman & Taylor, 1973; Laurenceau et al., 1998; Reis & Shaver, 1988).
This is why many non-autistics’ needs for reciprocal sharing, for the continuous exchange of inner experience, is not a social preference or a personality trait. It is a structural feature of how the intimacy mechanism runs. The oscillation that drives all non-autistic development requires something to move against. In the domain of intimacy, what it moves against is the genuine presence of another person's inner world. The self-disclosure that flows toward the other and the reception that flows back are the same oscillation that has been running since infancy, now organized around the question of mutual knowing (Erikson, 1968; Laurenceau et al., 1998; Reis & Shaver, 1988).
There is something worth naming precisely here, because it matters for what happens when this process meets a different intimacy system. When non-autistic people share their self-reflections, the ideas and experiences they have developed through the continuous social mirroring that builds the non-autistic self-concept, they are sharing something deeply personal about how they have come to understand themselves. Those reflections are built from the outside-in formation that identity depends on: they carry the traces of how the social world has been received and integrated. To share them is to offer the product of that formation, which is to say, something of the self's own history of being known. What the non-autistic person is extending, in other words, is not merely a thought. It is an invitation into the process through which they became who they are (Erikson, 1968; Laurenceau et al., 1998; Reis et al., 2017).
The High Body Empathetic's Intimacy Challenge
Within the range of people whose development follows the non-autistic pathway, the high body empathetic, in MacMillan's theoretical framework, faces a specific and particular intimacy challenge. The nervous system that is exceptionally oriented toward others' experience, that registers another person's emotional states with unusual vividness and immediacy, is in some respects ideally designed for the intimacy process: it receives disclosures deeply, responds with genuine attunement, and creates in the other person the felt sense of being genuinely held (Craig, 2009; Critchley et al., 2004; Decety & Jackson, 2004; Lamm et al., 2007; Singer et al., 2004).
But genuine intimacy, as the opening post in this series established, requires two distinct selves. Contact, not merger (Erikson, 1968; Kegan, 1982). And for the high body empathetic, the very quality that makes them so capable of genuine reception creates a structural risk at the other end of the intimacy process: the self that is receiving so fully may find it difficult to maintain its own ground while doing so (Kegan, 1982; Reis & Shaver, 1988).
When the high body empathetic person is in genuine intimacy with another, the boundary between their own emotional experience and the other person's may become difficult to hold. The accommodation that runs strongly in this nervous system, the readiness to reorganize around what is present in the other person, can tip the intimacy process past genuine contact and into something closer to absorption (Craig, 2009; Kegan, 1982; Lamm et al., 2007). The self knows the other's experience vividly, deeply, and empathically. But the other's experience begins to fill the relational space in a way that makes the high body empathetic's own experience progressively harder to locate.
This is not a failure of intimacy. It is intimacy's particular challenge for this nervous system: staying grounded in one's own experience while remaining genuinely open to another's, bringing oneself into genuine contact rather than dissolving the self in the encounter (Erikson, 1968; Kegan, 1982). The developmental work for the high body empathetic in the domain of intimacy is the assimilative work described in the identity series: building the capacity to remain in one's own shoes, to stay present to one's own inner experience as a distinct thing, even in the presence of another person whose experience the nervous system is already fully inhabiting.
What the Non-Autistic Pathway Needs
What the non-autistic pathway needs in order for genuine intimacy to form is what the oscillation has always needed: a genuine exchange in which both movements complete. The self extends toward the other through disclosure, and the other receives it in a way that makes the extending feel worthwhile and safe. The other extends in return, and the self receives that extension genuinely. The back-and-forth accumulates over time into the experience of being known, and of knowing (Altman & Taylor, 1973; Laurenceau et al., 1998; Reis & Shaver, 1988).
For this to happen, the non-autistic person needs a partner who can receive their disclosures as the intimacy bids they are rather than as information to be processed or problems to be solved. They need the felt sense that their inner world matters to the person they are trying to be close to, that what they share has genuine impact, that the other person is actually present to them rather than managing them from a comfortable distance (Laurenceau et al., 1998; Reis & Gable, 2015; Reis et al., 2017).
And they need the conditions that allow the oscillation itself to remain calibrated: relationships and environments that provide neurotype-matched reciprocal disclosure, so that the intimacy the primary relationship can provide is received in a context of genuine relational fullness rather than deprivation (Crompton, Hallett, et al., 2020; Crompton, Sharp, et al., 2020; Sala et al., 2020).
What they need most, in the end, is what the intimacy process itself describes: to extend themselves genuinely, to be genuinely received, and to find in that reception the confirmation that the self they brought into contact was the self that was there to be known (Laurenceau et al., 1998; Reis & Shaver, 1988).
The autistic pathway approaches this same destination through a different structure entirely. What it needs from the intimacy process, and what it offers in return, is genuinely different from what the non-autistic pathway describes. That is where the next post turns.
Next in this series: How Intimacy Forms Along the Autistic Pathway, what autistic people want and are capable of in close relationship, the different channels through which autistic intimacy builds, and why same-neurotype connection so often produces the experience of finally being understood.
THE SERIES:
Article 1: What Intimacy Actually Is
Article 2: How Intimacy Forms Along the Non-Autistic Pathway
Article 3: How Intimacy Forms Along the Autistic Pathway
Article 4: Physical Intimacy, Sensory Experience and the Body
Article 5: When Two Intimacy Systems Meet
Article 6: Toward Mutual Intelligibility
References
Altman, I., & Taylor, D. A. (1973). Social penetration: The development of interpersonal relationships. Holt, Rinehart & Winston.
Craig, A. D. (2009). How do you feel—now? The anterior insula and human awareness. Nature Reviews Neuroscience, 10(1), 59–70. https://doi.org/10.1038/nrn2555
Critchley, H. D., Wiens, S., Rotshtein, P., Öhman, A., & Dolan, R. J. (2004). Neural systems supporting interoceptive awareness. Nature Neuroscience, 7(2), 189–195. https://doi.org/10.1038/nn1176
Crompton, C. J., Hallett, S., Ropar, D., Flynn, E. G., & Fletcher-Watson, S. (2020). “I never realised everybody felt as happy as I do when I am around autistic people”: A thematic analysis of autistic adults’ relationships with autistic and neurotypical friends and family. Autism, 24(6), 1438–1448. https://doi.org/10.1177/1362361320908976
Crompton, C. J., Sharp, M., Axbey, H., Fletcher-Watson, S., Flynn, E. G., & Ropar, D. (2020). Neurotype-matching, but not being autistic, influences self and observer ratings of interpersonal rapport. Frontiers in Psychology, 11, Article 586171. https://doi.org/10.3389/fpsyg.2020.586171
Decety, J., & Jackson, P. L. (2004). The functional architecture of human empathy. Behavioral and Cognitive Neuroscience Reviews, 3(2), 71–100. https://doi.org/10.1177/1534582304267187
Erikson, E. H. (1968). Identity: Youth and crisis. W. W. Norton.
Gallese, V. (2009). Mirror neurons, embodied simulation, and the neural basis of social identification. Psychoanalytic Dialogues, 19(5), 519–536. https://doi.org/10.1080/10481880903231910
Kegan, R. (1982). The evolving self: Problem and process in human development. Harvard University Press.
Lamm, C., Batson, C. D., & Decety, J. (2007). The neural substrate of human empathy: Effects of perspective-taking and cognitive appraisal. Journal of Cognitive Neuroscience, 19(1), 42–58. https://doi.org/10.1162/jocn.2007.19.1.42
Laurenceau, J.-P., Barrett, L. F., & Pietromonaco, P. R. (1998). Intimacy as an interpersonal process: The importance of self-disclosure, partner disclosure, and perceived partner responsiveness in interpersonal exchanges. Journal of Personality and Social Psychology, 74(5), 1238–1251. https://doi.org/10.1037/0022-3514.74.5.1238
Niedenthal, P. M. (2007). Embodying emotion. Science, 316(5827), 1002–1005. https://doi.org/10.1126/science.1136930
Reis, H. T., & Gable, S. L. (2015). Responsiveness. Current Opinion in Psychology, 1, 67–71. https://doi.org/10.1016/j.copsyc.2015.01.001
Reis, H. T., Lemay, E. P., Jr., & Finkenauer, C. (2017). Toward understanding understanding: The importance of feeling understood in relationships. Social and Personality Psychology Compass, 11(3), Article e12308. https://doi.org/10.1111/spc3.12308
Reis, H. T., & Shaver, P. (1988). Intimacy as an interpersonal process. In S. Duck, D. F. Hay, S. E. Hobfoll, W. Ickes, & B. M. Montgomery (Eds.), Handbook of personal relationships: Theory, research and interventions (pp. 367–389). Wiley.
Sala, G., Hooley, M., & Stokes, M. A. (2020). Romantic intimacy in autism: A qualitative analysis. Journal of Autism and Developmental Disorders, 50, 4133–4147. https://doi.org/10.1007/s10803-020-04377-x
Singer, T., Seymour, B., O’Doherty, J. P., Kaube, H., Dolan, R. J., & Frith, C. D. (2004). Empathy for pain involves the affective but not sensory components of pain. Science, 303(5661), 1157–1162. https://doi.org/10.1126/science.1093535

© 2023 REAL Neurodiverse
All Rights Reserved
anne@neurodiversemarriage.com
Text or Call: (617) 996-7239 (United States)