DPR
Dissociated Pain Release
A self-help technique developed by a trauma survivor

Anne MacMillan, MLA
Survivor, Consultant, Coach
Master's Clinical Psychology - Harvard University
Dissociated Pain Release
Self-Help Trauma Support
Dissociated Pain Release
Dissociated Pain Release (DPR) is a self-help technique that allows users to release emotional pain from trauma without re-experiencing it. It is based on the idea that emotional pain is stored in the mind, body, and nervous system and that the stored pain causes distress and discomfort in the present, whether the trauma was a recent event or something that happened many years ago.
There is no need for a DPR user to know where any emotional pain came from. All a user needs to know is that they are currently experiencing unwanted emotional pain and that they would like to release that pain and feel better -- quickly.
Most importantly, in DPR, emotional pains are released while the user is dissociated from them -- allowing the user to process any trauma or distress without being forced to relive the original traumatic experience.
Examples of emotional pain that can be released from the body and nervous system through DPR include rage, anger, shame, sadness, guilt, grief, loneliness, abandonment, anxiety, and fear.
Likewise, DRP allows users to release any stored sensations associated with physical pain or forms of bodily discomfort that happened in the past. DPR users can release sensations of nausea, dizziness, cold, being drugged, etc. Again, all these sensations are released without the DRP user re-experiencing the original potency of any traumatic event. Often DPR users release pain without even knowing what the original traumatic event may have been.
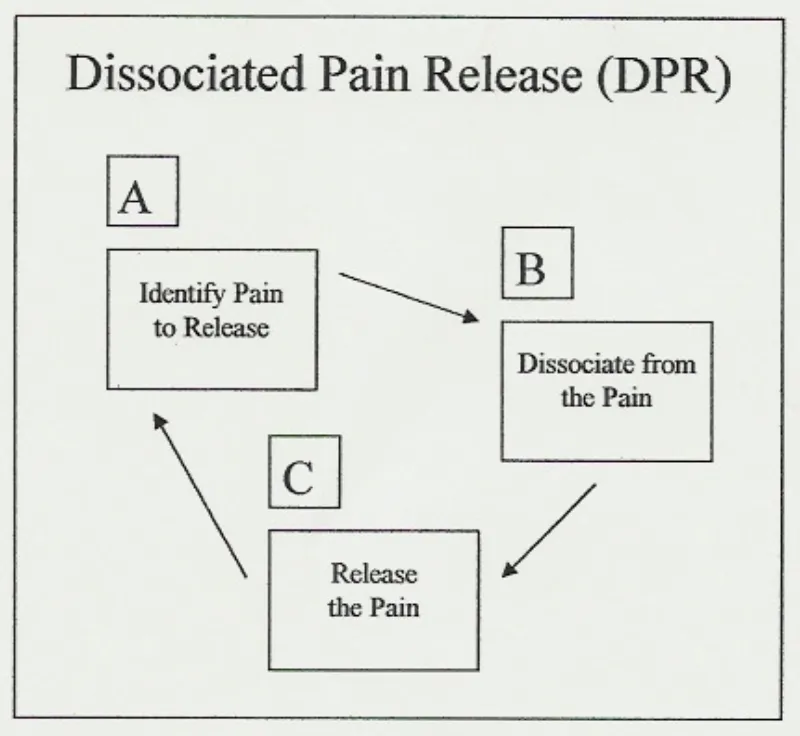
DPR has three cyclical steps: (A) identify pain to release, (B) dissociate from the pain, and (C) release the pain. Once understood, DPR is a simple, repetitive process that applies in many self-help situations. Any user employing DPR expects to complete its A-B-C cycle several times in any one self-help session. It is understood that there may be several painful emotions, different forms of physical pain and other negative bodily sensations that require release, making time and repetition necessary.
IMPORTANT
* DPR is not trauma therapy.
Anne is not a therapist and does not support individuals through trauma therapy. Anne teaches a self-help technique that individuals can apply to many situations in their everyday lives and that they have a right to use to manage any experiences they choose, traumatic or not. It is always recommended that trauma survivors hire a licensed trauma therapists whenever possible. Call 911 in any emergency.
Feeling Suicidal?
Find a Helpline

Anne MacMillan, MLA
Survivor, Consultant, Coach, Educator
Master's Clinical Psychology, Harvard Univerisity
IMPORTANT
* DPR is not trauma therapy.
Anne is not a therapist and does not support individuals through trauma therapy. Anne teaches a self-help technique that individuals can apply to many situations in their everyday lives and that they have a right to use to manage any experiences they choose, traumatic or not.
It is always recommended that trauma survivors hire a licensed trauma therapists whenever possible. Call 911 in any emergency.
Feeling Suicidal?
Find a Helpline:
https://findahelpline.com/
About Me
Like many others, I grew up in a household that didn't offer me the basic protections all children need. I experienced extreme trauma as a very young child and, unfortunately, that trauma continued into my adolescence and adulthood.
I survived adolescence emotionally by focusing on studying contemporary dance, helping me process my emotions and increase my body awareness. As a young adult in my twenties, I was exposed to relaxation and meditation techniques and the idea that healing that comes naturally when we move our eyes as we dream.
In my mid-twenties, memories of traumatic events that had happened during my early childhood began to return to my consciousness. I knew about EMDR (Eye-Movement Desensitization and Reprocessing) therapy for trauma, but wasn't in a situation that allowed me consistent access to a trauma therapist.
So, I began working through my traumatic memories on my own, combining what I'd learned about the emotions I felt in my body through dancing with relaxation and visualization techniques. I added what I decided to call REM Simulation -- or Rapid Eye Movement Simulation. REM sleep is the deep dreaming sleep in which humans naturally process emotions.
The result was a self-help technique that made it possible for me to work through the terrible emotions associated with traumatic events that had occurred in my past and regain the sense of emotional stability I needed -- all without having an opportunity to get the therapeutic support I needed.
Dissociated Pain Release
I dubbed my self-help technique DPR, or Dissociated Pain Release, and decided that I didn't want it to ever become something that anyone with an advanced degree and a lot of privilege could tell people they weren't qualified to perform at home on their own.
Therapy is wonderful and everyone who has access to a therapist should take advantage of that privilege. But recovery strategies should be available to anyone anywhere. That's what DPR is about for me.
From my perspective, DPR is nothing more than a collection of practical ideas put together in one package to help all of us get through the difficult emotions humans feel. It's valuable because it works and it uses human's natural REM (Rapid Eye Movement) sleep processing methods.

My Newest Blog Posts

Physical Intimacy, Sensory Experience, and the Body
Series V, Article 4: Physical Intimacy, Sensory Experience, and the Body
Physical intimacy is not simply emotional intimacy with bodies involved. It is its own domain, with its own specific requirements, its own particular vulnerabilities, and its own relationship to the question this series is organized around: what does genuine closeness require, and what does it produce? Treating physical intimacy as merely the embodied version of the emotional intimacy the previous posts described would miss something essential. The body is not a passive channel through which emotional connection flows. It is an active participant in the intimacy process, carrying its own information, its own language, and its own conditions for safety (Laurenceau et al., 1998; Reis & Shaver, 1988; Sala et al., 2024).
Understanding what physical intimacy is and does, across different neurological architectures, requires taking seriously what different nervous systems actually experience when bodies are in proximity, in contact, and in the particular kind of vulnerable closeness that physical intimacy represents (Crane et al., 2009; Gray et al., 2021; Sala et al., 2024).
What the Body Does in Non-Autistic Intimacy
For many people whose development follows the non-autistic pathway, physical closeness is not neutral. It carries emotional information automatically, through the same body empathy channels that carry all social and emotional information: the continuous, embodied, largely automatic reception of what another person is experiencing through their body (Craig, 2009; Critchley et al., 2004; Decety & Jackson, 2004). When two non-autistic people are in physical proximity, body empathy means they are registering each other's states in real time, not through deliberate attention but through the nervous system's automatic orientation toward the social field (Craig, 2009; Decety & Jackson, 2004).
Physical contact, in this context, functions as one of the most direct channels through which the non-autistic intimacy process runs. Touch, proximity, shared physical space: all of these carry emotional meaning that arrives immediately and below the level of conscious awareness (Craig, 2009; Decety & Jackson, 2004; Laurenceau et al., 1998). Physical closeness can confirm felt connection, can repair relational disruption, can communicate care and commitment in ways that verbal exchange does not always reach. For many non-autistic people, physical intimacy serves as embodied confirmation of attachment, the sense of being securely held by another person made tangible through physical contact, which carries a different and in some ways more immediate emotional weight than words (Byers et al., 2013; Laurenceau et al., 1998; Sala et al., 2024).
This means that for the non-autistic pathway, physical and emotional intimacy are closely interwoven, each feeding and amplifying the other. The body is part of the intimacy mechanism rather than a separate domain from it. And the absence of physical intimacy in a relationship, or physical intimacy that feels disconnected from emotional meaning, can represent a specific kind of relational loss that the non-autistic nervous system registers acutely (Byers et al., 2013; Laurenceau et al., 1998; Reis & Shaver, 1988).
Sensory Processing and What Physical Closeness Actually Means
For people whose development follows the autistic pathway, the sensory experience of physical contact is more variable, more determining of what physical closeness actually means, and less automatically organized around the emotional meaning that the non-autistic template attaches to it (Crane et al., 2009; Gray et al., 2021; Sala et al., 2024).
Autistic people's sensory processing often differs from non-autistic norms in ways that are specific to the individual: heightened sensitivity to particular kinds of touch, particular textures, temperatures, or pressures; differences in how the nervous system processes unexpected contact versus anticipated contact; differences in how sensory input accumulates over time and what happens when it exceeds a particular threshold (Crane et al., 2009; Gray et al., 2021; Maggio et al., 2022). These are not preferences in the ordinary sense of the word, things one might override with sufficient motivation. They are features of the nervous system's processing architecture, and they shape the experience of physical contact in ways that are genuinely determining of what physical closeness means in any given moment (Crane et al., 2009; Gray et al., 2021).
This means that the same touch that communicates warmth and security to one person may communicate overwhelm, intrusion, or something closer to pain to another. The same physical proximity that creates felt connection for a non-autistic nervous system may create sensory demand for an autistic nervous system, and sensory demand, even when it is not aversive, requires attention and processing that can make the emotional presence that physical intimacy is supposed to facilitate genuinely harder to access (Crane et al., 2009; Gray et al., 2021; Sala et al., 2024). The body is occupied with managing the sensory experience rather than with being present to the relational one.
It is important to say clearly: none of this means that autistic people do not want physical closeness, or that physical intimacy is not important or meaningful for autistic people. What the research consistently finds is that autistic people's experience of physical intimacy is more variable than the non-autistic template assumes, more dependent on specific sensory conditions, more influenced by predictability and context, and less organized around a single default meaning that physical contact is supposed to carry (Barnett & Maticka-Tyndale, 2015; Byers et al., 2013; Gray et al., 2021; Sala et al., 2024). For some autistic people, physical intimacy is central and deeply wanted. For others, it occupies a different place in the relational landscape. For many, what makes physical closeness genuinely connecting is specific to their individual sensory profile and the particular conditions of a particular encounter with a particular person, built across time (Byers et al., 2013; Gray et al., 2021; Sala et al., 2024).
Sensory Safety as a Prerequisite
What emerges from taking sensory processing seriously in the context of physical intimacy is a concept worth naming explicitly: sensory safety. Sensory safety, in the context of physical closeness, is the condition in which the sensory experience of physical contact is sufficiently within the person's nervous system's processing capacity that genuine presence in the encounter is possible (Crane et al., 2009; Gray et al., 2021; Sala et al., 2024).
This is not an accommodation to be granted or a clinical modification to be made. It is a precondition. Physical intimacy can only function as a pathway toward genuine closeness if the person being touched is actually present in the experience rather than managing it. An autistic person who is in physical contact that exceeds their sensory threshold is not available for the relational experience the contact is intended to create. They are available for the sensory experience, which is a different and more consuming thing (Crane et al., 2009; Gray et al., 2021).
Sensory safety requires knowing what creates it for the specific person: which kinds of touch are welcome, which are overwhelming, which are neutral, and how those responses shift depending on context, timing, the state of the nervous system's arousal, and the accumulated sensory load of the day (Crane et al., 2009; Gray et al., 2021; Sala et al., 2024). It requires that this knowledge be available in the relationship, which means it has to be explicitly communicated and explicitly received, because the non-autistic nervous system does not automatically detect when physical contact has moved from connecting to demanding. Body empathy reads emotional states, not sensory processing states, and the two can diverge substantially (Craig, 2009; Critchley et al., 2004; Gray et al., 2021).
Physical Intimacy as Explicit Practice
Here is where the physical intimacy domain offers something that is, once properly understood, genuinely valuable rather than merely challenging: the necessity of explicit conversation about physical intimacy creates the conditions for physical closeness to be precisely calibrated to what each person's nervous system actually needs and genuinely welcomes (Barnett & Maticka-Tyndale, 2015; Gray et al., 2021; Sala et al., 2024).
Non-autistic physical intimacy often unfolds through implicit reading of embodied signals: body empathy registering whether closeness is welcome, adjusting in real time to what the other person's body is communicating, negotiating the terms of physical contact through a continuous nonverbal exchange that neither person has to make conscious or deliberate (Craig, 2009; Decety & Jackson, 2004; Laurenceau et al., 1998). This can be profound when both nervous systems are reading from the same script. When they are not, the implicit negotiation fails, and the failure may not be noticed until well after the fact (Jones et al., 2024; Milton, 2012; Yew et al., 2023).
Explicit conversation about physical intimacy, about what kinds of contact are welcoming for each person, about what timing and predictability and pace create the conditions for genuine presence, about how sensory needs shift and how to communicate that shift in real time, is not the absence of spontaneity. It is the creation of the specific conditions under which genuine physical closeness becomes possible (Barnett & Maticka-Tyndale, 2015; Gray et al., 2021; Sala et al., 2024). For autistic people especially, but in reality for both people in any relationship where sensory architectures differ, knowing what physical intimacy means for the other person and being known in return about what it means for oneself is an intimate act in itself: an act of genuine disclosure and genuine reception, which is the intimacy process this series has been describing at its most essential (Laurenceau et al., 1998; Reis & Shaver, 1988).
Explicit practice in physical intimacy also means something that extends beyond sensory preferences: communicating clearly about desire and readiness itself. One person's desire for physical closeness carries no automatic information about a partner's. For the non-autistic nervous system, body empathy provides continuous feedback about a partner's interest, availability, and willingness, and the implicit negotiation that non-autistic physical intimacy relies on depends on that feedback being available and legible (Craig, 2009; Decety & Jackson, 2004). When the autistic nervous system does not automatically receive that feedback, the subtle non-verbal signals through which a partner communicates hesitation, discomfort, or unwillingness may not register as the refusal they are (Jones et al., 2024; Milton, 2012). The autistic person may be genuinely unaware that a limit is being crossed, and the harm that follows is real regardless of intent. Explicit communication about readiness and desire, in language that is verbal and unambiguous rather than carried through non-verbal channels the autistic nervous system may not automatically read, is not a formality. It is what makes physical intimacy genuinely safe (Barnett & Maticka-Tyndale, 2015; Maggio et al., 2022; Motamed et al., 2025; Sala et al., 2024).
In neurodiverse relationships, where two nervous systems with different sensory architectures and different default meanings for physical contact are trying to find shared ground, explicit practice is how physical intimacy becomes genuinely available to both people, because each person's experience of physical closeness is organized around assumptions the other does not automatically share, and what creates connection for one person is not automatically what creates it for the other (Gray et al., 2021; Milton, 2012; Sala et al., 2024; Yew et al., 2023).
What Physical Intimacy Can Be
When the conditions are right, physical intimacy does something that no other form of intimacy quite replicates: it confirms genuine knowing in the body. The person whose specific sensory needs have been attended to, whose particular ways of welcoming contact have been learned and honored, experiences in physical closeness something that goes beyond the emotional intimacy the previous posts described. They experience being known through the body: the other person's attention to what their nervous system actually requires is itself a form of seeing, a recognition of who they specifically are rather than who a generic body is assumed to be (Gray et al., 2021; Laurenceau et al., 1998; Sala et al., 2024).
This is available across both developmental pathways, though it requires different things from each. For the non-autistic pathway, it requires the willingness to move from implicit negotiation to explicit conversation, to make deliberate what body empathy might otherwise handle automatically, and to remain genuinely attentive to a partner's sensory experience rather than assuming the emotional meaning of contact is shared (Craig, 2009; Decety & Jackson, 2004; Gray et al., 2021).
For the autistic pathway, it requires the courage to name what the sensory experience actually is, which requires both self-knowledge and enough felt safety in the relationship that the naming does not feel like an imposition on the connection (Gray et al., 2021; Sala et al., 2024). It also requires recognizing that one's own desire for physical closeness carries no automatic information about a partner's: without the body empathy feedback loop, signals of unwillingness or unreadiness can be genuinely missed, and the consequences of that gap can be serious (Jones et al., 2024; Milton, 2012). Explicit yes and explicit no, rather than the non-verbal signals the autistic nervous system may not automatically receive, are what makes physical intimacy safe for both people (Maggio et al., 2022; Motamed et al., 2025).
When both are present, what physical intimacy produces is genuine. Two people, known to each other in their specific and particular bodies, closing the distance between them in a way that neither loses themselves in nor protects themselves from. Contact rather than merger, presence rather than performance (Laurenceau et al., 1998; Reis & Shaver, 1988; Sala et al., 2024).
That is what physical intimacy is reaching for. It is the body's contribution to the question this series has been asking: what does it mean to genuinely know and be known by another person?
Next in this series: When Two Intimacy Systems Meet, what happens in neurodiverse relationships when the non-autistic and autistic approaches to intimacy encounter each other, what each person is offering and what each person is waiting for, and why two people who genuinely care for each other can still be profoundly lonely in the same relationship.
THE SERIES:
Article 1: What Intimacy Actually Is
Article 2: How Intimacy Forms Along the Non-Autistic Pathway
Article 3: How Intimacy Forms Along the Autistic Pathway
Article 4: Physical Intimacy, Sensory Experience and the Body
Article 5: When Two Intimacy Systems Meet
Article 6: Toward Mutual Intelligibility
References
Barnett, J. P., & Maticka-Tyndale, E. (2015). Qualitative exploration of sexual experiences among adults on the autism spectrum: Implications for sexuality education. Perspectives on Sexual and Reproductive Health, 47(4), 171–179. https://doi.org/10.1363/47e5715
Byers, E. S., Nichols, S., Voyer, S. D., & Reilly, G. (2013). Sexual well-being of a community sample of high-functioning adults on the autism spectrum who have been in a romantic relationship. Autism, 17(4), 418–433. https://doi.org/10.1177/1362361311431950
Craig, A. D. (2009). How do you feel—now? The anterior insula and human awareness. Nature Reviews Neuroscience, 10(1), 59–70. https://doi.org/10.1038/nrn2555
Crane, L., Goddard, L., & Pring, L. (2009). Sensory processing in adults with autism spectrum disorders. Autism, 13(3), 215–228. https://doi.org/10.1177/1362361309103794
Critchley, H. D., Wiens, S., Rotshtein, P., Öhman, A., & Dolan, R. J. (2004). Neural systems supporting interoceptive awareness. Nature Neuroscience, 7(2), 189–195. https://doi.org/10.1038/nn1176
Decety, J., & Jackson, P. L. (2004). The functional architecture of human empathy. Behavioral and Cognitive Neuroscience Reviews, 3(2), 71–100. https://doi.org/10.1177/1534582304267187
Gray, S., Kirby, A. V., & Graham Holmes, L. (2021). Autistic narratives of sensory features, sexuality, and relationships. Autism in Adulthood, 3(3), 238–246. https://doi.org/10.1089/aut.2020.0049
Jones, D. R., Botha, M., Ackerman, R. A., King, K., & Sasson, N. J. (2024). Non-autistic observers both detect and demonstrate the double empathy problem when evaluating interactions between autistic and non-autistic adults. Autism, 28(8), 2053–2065. https://doi.org/10.1177/13623613231219743
Laurenceau, J.-P., Barrett, L. F., & Pietromonaco, P. R. (1998). Intimacy as an interpersonal process: The importance of self-disclosure, partner disclosure, and perceived partner responsiveness in interpersonal exchanges. Journal of Personality and Social Psychology, 74(5), 1238–1251. https://doi.org/10.1037/0022-3514.74.5.1238
Maggio, M. G., Calatozzo, P., Cerasa, A., Pioggia, G., Quartarone, A., & Calabrò, R. S. (2022). Sex and sexuality in autism spectrum disorders: A scoping review on a neglected but fundamental issue. Brain Sciences, 12(11), Article 1427. https://doi.org/10.3390/brainsci12111427
Milton, D. E. M. (2012). On the ontological status of autism: The “double empathy problem.” Disability & Society, 27(6), 883–887. https://doi.org/10.1080/09687599.2012.710008
Motamed, M., Hajikarim-Hamedani, A., Fakhrian, A., & Alaghband-rad, J. (2025). A systematic review of sexual health, knowledge, and behavior in autism spectrum disorder. BMC Psychiatry, 25, Article 410. https://doi.org/10.1186/s12888-025-06836-x
Reis, H. T., & Shaver, P. (1988). Intimacy as an interpersonal process. In S. Duck, D. F. Hay, S. E. Hobfoll, W. Ickes, & B. M. Montgomery (Eds.), Handbook of personal relationships: Theory, research and interventions (pp. 367–389). Wiley.
Sala, G., Hooley, J., Hooley, M., & Stokes, M. A. (2024). Comparing physical intimacy and romantic relationships of autistic and non-autistic adults: A qualitative analysis. Journal of Autism and Developmental Disorders, 54, 3942–3951. https://doi.org/10.1007/s10803-023-06109-0
Yew, R. Y., Hooley, M., & Stokes, M. A. (2023). Factors of relationship satisfaction for autistic and non-autistic partners in long-term relationships. Autism, 27(8), 2348–2360. https://doi.org/10.1177/13623613231160244

© 2023 REAL Neurodiverse
All Rights Reserved
anne@neurodiversemarriage.com
Text or Call: (617) 996-7239 (United States)