DPR
Dissociated Pain Release
A self-help technique developed by a trauma survivor

Anne MacMillan, MLA
Survivor, Consultant, Coach
Master's Clinical Psychology - Harvard University
Dissociated Pain Release
Self-Help Trauma Support
Dissociated Pain Release
Dissociated Pain Release (DPR) is a self-help technique that allows users to release emotional pain from trauma without re-experiencing it. It is based on the idea that emotional pain is stored in the mind, body, and nervous system and that the stored pain causes distress and discomfort in the present, whether the trauma was a recent event or something that happened many years ago.
There is no need for a DPR user to know where any emotional pain came from. All a user needs to know is that they are currently experiencing unwanted emotional pain and that they would like to release that pain and feel better -- quickly.
Most importantly, in DPR, emotional pains are released while the user is dissociated from them -- allowing the user to process any trauma or distress without being forced to relive the original traumatic experience.
Examples of emotional pain that can be released from the body and nervous system through DPR include rage, anger, shame, sadness, guilt, grief, loneliness, abandonment, anxiety, and fear.
Likewise, DRP allows users to release any stored sensations associated with physical pain or forms of bodily discomfort that happened in the past. DPR users can release sensations of nausea, dizziness, cold, being drugged, etc. Again, all these sensations are released without the DRP user re-experiencing the original potency of any traumatic event. Often DPR users release pain without even knowing what the original traumatic event may have been.
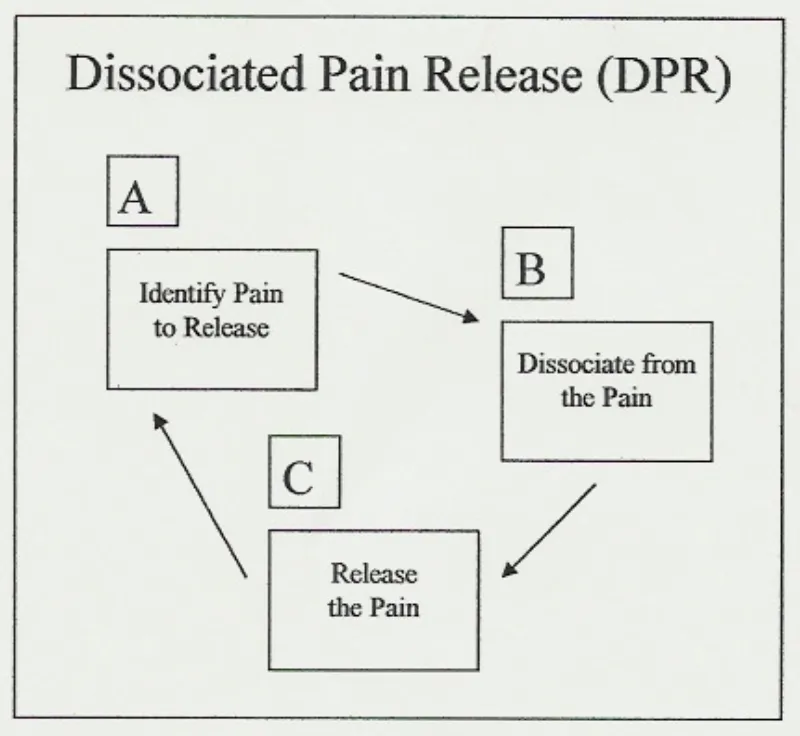
DPR has three cyclical steps: (A) identify pain to release, (B) dissociate from the pain, and (C) release the pain. Once understood, DPR is a simple, repetitive process that applies in many self-help situations. Any user employing DPR expects to complete its A-B-C cycle several times in any one self-help session. It is understood that there may be several painful emotions, different forms of physical pain and other negative bodily sensations that require release, making time and repetition necessary.
IMPORTANT
* DPR is not trauma therapy.
Anne is not a therapist and does not support individuals through trauma therapy. Anne teaches a self-help technique that individuals can apply to many situations in their everyday lives and that they have a right to use to manage any experiences they choose, traumatic or not. It is always recommended that trauma survivors hire a licensed trauma therapists whenever possible. Call 911 in any emergency.
Feeling Suicidal?
Find a Helpline

Anne MacMillan, MLA
Survivor, Consultant, Coach, Educator
Master's Clinical Psychology, Harvard Univerisity
IMPORTANT
* DPR is not trauma therapy.
Anne is not a therapist and does not support individuals through trauma therapy. Anne teaches a self-help technique that individuals can apply to many situations in their everyday lives and that they have a right to use to manage any experiences they choose, traumatic or not.
It is always recommended that trauma survivors hire a licensed trauma therapists whenever possible. Call 911 in any emergency.
Feeling Suicidal?
Find a Helpline:
https://findahelpline.com/
About Me
Like many others, I grew up in a household that didn't offer me the basic protections all children need. I experienced extreme trauma as a very young child and, unfortunately, that trauma continued into my adolescence and adulthood.
I survived adolescence emotionally by focusing on studying contemporary dance, helping me process my emotions and increase my body awareness. As a young adult in my twenties, I was exposed to relaxation and meditation techniques and the idea that healing that comes naturally when we move our eyes as we dream.
In my mid-twenties, memories of traumatic events that had happened during my early childhood began to return to my consciousness. I knew about EMDR (Eye-Movement Desensitization and Reprocessing) therapy for trauma, but wasn't in a situation that allowed me consistent access to a trauma therapist.
So, I began working through my traumatic memories on my own, combining what I'd learned about the emotions I felt in my body through dancing with relaxation and visualization techniques. I added what I decided to call REM Simulation -- or Rapid Eye Movement Simulation. REM sleep is the deep dreaming sleep in which humans naturally process emotions.
The result was a self-help technique that made it possible for me to work through the terrible emotions associated with traumatic events that had occurred in my past and regain the sense of emotional stability I needed -- all without having an opportunity to get the therapeutic support I needed.
Dissociated Pain Release
I dubbed my self-help technique DPR, or Dissociated Pain Release, and decided that I didn't want it to ever become something that anyone with an advanced degree and a lot of privilege could tell people they weren't qualified to perform at home on their own.
Therapy is wonderful and everyone who has access to a therapist should take advantage of that privilege. But recovery strategies should be available to anyone anywhere. That's what DPR is about for me.
From my perspective, DPR is nothing more than a collection of practical ideas put together in one package to help all of us get through the difficult emotions humans feel. It's valuable because it works and it uses human's natural REM (Rapid Eye Movement) sleep processing methods.

My Newest Blog Posts

How the R.E.A.L. Neurodiverse™ 10-Step Approach Moves Clients From Confusion to Clarity
Section 1: Why Neurodiverse Family Systems Need a Structured Pathway
Providers who work with neurodiverse families often encounter a particular kind of clinical disorientation that is worth naming directly. The presenting picture is rarely simple. A family may arrive carrying conflict, shutdown, emotional intensity, chronic avoidance, failed repair, trauma responses, and years of accumulated misinterpretation, all layered on top of neurological differences that no one in the system has ever had accurate language to describe. The pain is real and it is relational, and the instinct is to address it relationally. But the question of where to actually begin, what to address first, what the work is even trying to produce, can be genuinely difficult to answer without a framework that accounts for the specific mechanisms driving neurodiverse family distress.
Clients face a parallel version of the same disorientation. Family members who have spent years inside a neurodiverse system often arrive not knowing what is neurological and what is personal, what is changeable and what is not, what they are responsible for and what they have been carrying that was never theirs to carry. An autistic family member may have no framework for understanding how their sensory processing, cognitive load, or need for direct communication has been shaping the relational environment around them (Mahler et al., 2022). A high body empathetic family member may know they are exhausted but have no language for why absorbing the emotional states of everyone in the system has become the organizing fact of their daily life (Gallese, 2009). An attention neurodivergent family member may have spent years being experienced by others as unreliable or careless without understanding the executive function realities underneath that perception (Shaw et al., 2014). A neurotypical family member may be interpreting everything through assumptions that feel like common sense but are, in fact, neurologically specific in ways they have never been asked to examine (Milton, 2012).
Without a structured pathway through that confusion, the work tends to follow the loudest signal. It moves from crisis to crisis, conflict to conflict, relational rupture to relational rupture, addressing the surface while the mechanisms underneath continue undisturbed. Clients may make genuine efforts and still find themselves in the same place. Providers may work hard and skillfully and still feel like the sessions are not gaining traction. The problem is not effort or intention. It is the absence of a structure that can hold the complexity of what neurodiverse family systems actually are and move through it in a sequence that matches how understanding, integration, and change actually develop.
This is what the R.E.A.L. Neurodiverse™ 10-Step Approach was built to provide. Not a rigid script, and not a one-size-fits-all intervention, but a structured pathway that gives providers and clients a way to move through the specific dimensions of neurodiverse family experience in a sequence that builds on itself, that protects individual process before introducing relational complexity, and that keeps clarity, rather than repair or reconciliation, at the center of the work.
At the heart of that pathway is a simple but carefully considered sequence that operates at every step and substep of the model: shared psychoeducation, individual integration, and optional relational discussion. Understanding why that sequence exists, and what each stage is actually designed to do, is the starting point for understanding how the approach works.
Section 2: The Three-Stage Insight Pathway
The Three-Stage Insight Pathway is not a preliminary structure that clients move through once before the real work begins. It is the architecture of the work itself, repeating at every step and substep of the R.E.A.L. Neurodiverse™ 10-Step Approach, each time at a greater depth and with more relational capacity than the pass before it. Understanding what each stage is designed to do, and why the sequence matters, is essential for providers who want to use the framework with the precision it was built to support.
Stage 1: Shared Psychoeducation
The first stage gives clients a common foundation. Before anyone can understand what is happening in a neurodiverse family system, they need accurate language for the mechanisms driving it. Without that language, family members are left interpreting each other through the only frameworks available to them, which are usually built on neurotypical assumptions about how relational signals should be sent and received, how emotional repair should work, and what a reasonable level of effort and responsiveness looks like. Those assumptions, applied to people whose neurologies operate differently, produce the misinterpretations that accumulate into the cycles, roles, and relational injuries that bring most neurodiverse families into the work in the first place (Milton, 2012).
Psychoeducation interrupts that process by replacing assumption with understanding (Oehme et al., 2024). It gives clients language for what has been happening underneath the behavior they have been trying to interpret for years. The word shared matters here, though not in the sense that everyone must learn together in the same room. It means that the educational foundation is consistent across the model, so that each client, regardless of their neurological profile, is working from the same conceptual framework. That shared framework is what eventually makes genuine relational understanding possible, not because everyone now agrees, but because everyone is finally looking at the same underlying reality.
What psychoeducation does not do, and this is as important as what it does, is resolve the confusion on its own. Knowing that a pattern has a neurological root does not automatically change how it feels to be on the receiving end of it. Knowing that a family member's withdrawal is sensory rather than punitive does not immediately dissolve the accumulated hurt of years of experiencing it as abandonment. Psychoeducation opens the door. The work that actually moves through it happens in Stage 2.
Stage 2: Individual Integration
Individual integration is the heart of the model. It is where psychoeducation becomes personal, where understanding moves from the conceptual level into the lived experience of a specific person with a specific neurology navigating a specific family system. And it is where the most clinically significant work often happens, regardless of whether Stage 3 ever follows.
The questions that individual integration is designed to support are not abstract. They are deeply personal. What does this understanding mean for me, in my family, in my history, in my body? How has my neurology been shaping my experience of the system, and how has the system been shaping my experience of my neurology? What patterns have I been pulled into, and what has kept me there? What have I been holding that was never mine to hold? What do I actually need, as distinct from what the system has required of me? What choices are genuinely available to me, and what am I still treating as fixed that might not be?
These questions require time, space, and a relational container that is organized entirely around the individual's own process, without the pull of other nervous systems, without the pressure of other people's needs and interpretations, and without the implicit demand to perform insight in a way that is legible or useful to anyone else in the family. For many autistic clients in particular, this kind of structured individual space is where they first gain genuine access to an accurate map of their own experience — research confirms that autistic self-awareness, when supported in the right conditions, becomes a foundation for more authentic engagement across all relational contexts (Bertilsdotter Rosqvist et al., 2023). And for many clients more broadly, it is the first time they have had access to a space that finally dissolves the self-blame that accumulated when frameworks couldn't explain what they were living (Corden et al., 2021).
It is also important to be clear about what individual integration is not. It is not a partial or preliminary use of the framework, a waiting room for the relational discussion that is assumed to be the real destination. For many clients, individual integration is the complete and sufficient use of the framework. A client who develops accurate self-understanding, recognizes the system patterns they have been part of, builds limits that are realistic and connected to action, makes decisions that improve their life, and stops measuring their own growth by whether the system changes in response, has not done incomplete work. They have done the work. The R.E.A.L. Neurodiverse™ Approach holds individual clarity as a full and meaningful outcome in its own right, not as a consolation prize for clients who were unable to reach relational discussion.
Stage 3: Optional Relational Discussion
The third stage offers the possibility of structured relational discussion between family members who are prepared, willing, and safe enough to engage in it. The word optional is not a soft qualifier. It is a clinical and ethical position that is non-negotiable within the framework.
Neurodiverse family systems frequently include serious harm. Some include emotional abuse, coercive control, chronic invalidation, trauma responses, and longstanding relational injuries that have left family members genuinely unsafe in each other's presence. In those situations, moving toward relational discussion is not a neutral clinical choice. It is a choice with consequences, and the consequences can include retraumatization, reinforcement of harmful dynamics, and the message, however unintended, that the harmed person's safety is less important than the system's opportunity for reconciliation. This is especially important to name clearly because emotional and psychological abuse — which involves no physical harm — is among the most underrecognized forms of relational danger and among the most likely to be minimized in clinical settings (Kassing & Collins, 2026). Research is unambiguous that conjoint therapy is contraindicated when coercive control or abuse is present, and proceeding without adequate safety assessment can cause significant harm (Karakurt et al., 2016).
Even in systems where serious harm is not present, relational discussion without adequate preparation tends to reproduce the cycles it was meant to interrupt. One person explains and another shuts down. One person seeks repair and another experiences pressure. One person discloses pain and another becomes defensive. The conversation that was supposed to produce something new runs on the oldest available version of the system's operating logic, because neither person has yet done the individual work that would allow them to stay in contact with themselves while also staying in contact with the other.
Stage 3 is available when the conditions are genuinely right: when both parties have moved through individual integration, when safety is established, when consent is fully informed and freely given, and when the structure of the discussion is designed to support insight and shared understanding rather than problem-solving or conflict resolution. Under those conditions, structured relational discussion can offer something that individual work alone cannot: the experience of being seen accurately by someone who shares the history, and of seeing them accurately in return. That experience, when it becomes possible, is genuinely valuable. But it is valuable because of the preparation that preceded it, not in spite of the absence of that preparation.
The sequence matters. And the optionality of Stage 3 is not a concession to difficulty. It is an acknowledgment of what neurodiverse family systems actually require in order for relational contact to be safe, honest, and genuinely useful to the people entering it.
Section 3: How the 10 Steps Organize the Work
The Three-Stage Insight Pathway is the repeating structure within each step of the R.E.A.L. Neurodiverse™ 10-Step Approach. The ten steps themselves are the larger architecture that determines what clients are learning and integrating as they move through that structure. Together, the steps and the pathway create something that neurodiverse family systems work has rarely had: a sequence that is specific enough to address the actual mechanisms driving family distress, and organized enough to build understanding gradually rather than all at once.
The approach begins with three foundational modules that sit before the ten steps and prepare clients for the work ahead. The first orients clients to neurodiversity itself. The second addresses the role that neurological difference plays in relational and family life. The third introduces the R.E.A.L. Neurodiverse™ 10-Step Approach as a framework, so that clients understand the structure they are moving through and why it is sequenced the way it is. These foundational modules are not administrative preliminaries. They establish the conceptual ground on which everything that follows is built, and clients who move through them with care arrive at Step 1 with significantly more capacity to do the individual integration work the steps require (Oehme et al., 2024).
Step 1 establishes wholeness and future orientation. It asks clients to begin from the premise that every person in the system is whole, that the distress in the family does not define the people in it, and that the work is oriented toward growth, clarity, and future possibility rather than toward diagnosis, blame, or the excavation of what went wrong. That orientation is not naive about the pain neurodiverse families carry. It is a deliberate clinical choice to anchor the work in what is possible rather than in what has already been lost.
Steps 2 and 3 move into the neurological core of the framework, and their sequence is deliberate. Step 2 asks clients to understand their own neurology first: how it shapes their perceptions, their needs, their strengths, their limits, their communication, and their relational patterns. Step 3 then expands that understanding outward to the neurologies of the people in the family system. That sequence matters because a person cannot accurately understand another's neurological reality until they have a clear and honest map of their own (Bertilsdotter Rosqvist et al., 2023). Asking clients to understand others before they understand themselves tends to produce empathy that is performed rather than grounded, accommodation that is reflexive rather than chosen, and interpretations of other people's behavior that are filtered through unexamined assumptions about what the client's own neurology treats as normal.
Step 4 addresses empathy differences, one of the most important and most misunderstood dimensions of neurodiverse family dynamics. Clients explore how empathy functions differently across neurologies, including differences in emotion-origin awareness, empathic-emotion intensity, interoception, and cognitive perspective-taking. Research confirms that cognitive and affective empathy are neurologically distinct capacities, and that different neurotypes show different profiles across these domains — findings that directly explain many of the persistent misattributions in neurodiverse family systems (Dziobek et al., 2008). For many clients, this step produces some of the most significant reframing of their relational history, because it replaces the assumption that one person cares more than another with an understanding of how different neurologies make caring available and visible in different ways.
Step 5 addresses something that neurodiverse family systems frameworks sometimes avoid: the reality that harmful narcissistic behaviors can occur across neurotypes. Autistic individuals and non-autistic individuals alike are capable of behavior that is harmful, coercive, or abusive, and accountability must not be replaced by either reflexive blame or diagnostic excuse. This step helps clients develop the capacity to hold both neurological understanding and genuine accountability at the same time, which is one of the more difficult clinical tasks in neurodiverse family systems work and one of the most necessary.
Step 6 introduces Neurodiverse Relationship Dynamics™, the recurring relational patterns that emerge when different neurologies interact over time. This is where the theoretical understanding developed in earlier steps begins to connect directly to the specific cycles and dynamics clients are living inside. Many clients find that the patterns described in this step match their own relational experience with a precision that earlier frameworks never came close to, and that recognition is itself a significant part of the work.
Step 7 addresses trauma, and specifically the ways trauma develops inside neurodiverse family systems. This is not only trauma in the conventional sense of discrete harmful events. It includes the accumulation of repeated misinterpretation, failed repair, and nervous system overwhelm that builds over years of neurological difference going unnamed and unaddressed (van der Kolk, 2014). Understanding how that accumulation becomes embedded in the nervous system, and how it shapes every subsequent relational interaction, is essential for clients who want to understand why change has felt so difficult and why the same patterns have kept reasserting themselves even after genuine effort.
Step 8 examines roles and their functions within the system. Every neurodiverse family develops roles, some consciously chosen, most not, that serve functions for the system as a whole (Kerr & Bowen, 1988). Understanding what role a person occupies, how it developed, what function it serves, and what it is costing the person who holds it is some of the most practically clarifying work the framework supports. It helps clients distinguish between what they have chosen and what they have been pulled into, and it opens the question of what it would mean to step out of a role the system has depended on.
Step 9 addresses cycles and intermittent trauma spikes, the recurring patterns of escalation, rupture, shutdown, and failed repair that organize so much of the daily experience of neurodiverse family life. Understanding how cycles form, what sustains them, and what conditions tend to produce the spikes that break through the surface of otherwise stable periods gives clients a way of reading their own relational history that replaces confusion and self-blame with something more accurate and more workable.
Step 10 considers development according to neurology. It asks how growth, identity, autonomy, intimacy, and relational capacity may unfold differently depending on neurological profile, and what that means for how clients understand their own development and the development of the people they are in relationship with (Corden et al., 2021). This step often produces a reframing of what progress looks like that is more honest, more neurology-affirming, and more useful than the developmental frameworks most clients have previously had access to.
Together, the ten steps move clients from the broadest possible orientation to neurodiverse family systems toward an increasingly specific and personal understanding of their own place within one. Each step builds on the last. The understanding developed at each stage makes the next stage more accessible, and the individual integration work at each step makes the relational discussions, when they occur, more grounded in reality and less organized around the accumulated confusion that brought the family into the work in the first place.
Section 4: Structure With Flexibility
A framework that is specific enough to be useful and flexible enough to be honest about the complexity of real clinical work is harder to build than it might appear. Specificity without flexibility produces rigidity, and rigidity in neurodiverse family systems work is not only unhelpful. It can replicate the very dynamic it is trying to address, imposing a predetermined structure on people whose neurologies have already spent years being asked to conform to frameworks that were not built for them. Flexibility without structure, on the other hand, produces drift, and drift in complex clinical work tends to follow the loudest signal rather than the most important one.
The R.E.A.L. Neurodiverse™ 10-Step Approach holds both. The sequential structure of the ten steps exists for a reason, and that reason is clinical rather than arbitrary. Neurodiverse family systems are complex enough that clients need a path through the material that builds understanding gradually, that establishes the foundation each subsequent step depends on, and that does not ask clients to understand others before they understand themselves, or to engage relationally before they have done the individual work that makes genuine relational engagement possible. The sequence is a recommendation grounded in how understanding actually develops in this specific kind of work, not a rule imposed from outside the clinical reality it is designed to serve.
At the same time, every client who comes to this work is their own unique person with their own neurological profile, their own history, their own relational context, and their own readiness. Some clients will need significantly more time in Step 2 than the structure might suggest, because understanding their own neurology is genuinely difficult and requires more than one pass through the material before it begins to feel personally real rather than intellectually interesting. Some clients will arrive with trauma that needs stabilization before any of the subsequent steps can be approached safely. Some clients will need boundary work, or crisis support, or grief work, before the family systems material can be engaged at the level of depth it requires. Some clients will move through certain steps quickly because the material resonates immediately with something they have already been trying to articulate for years, and will need more time at steps that touch something more defended or more painful.
Providers need to follow the client, not the framework. The framework exists to support that following, to give providers a map of the terrain and a sequence that reflects how the terrain is most productively navigated. But a map is not the same as the territory, and the territory of each individual client's experience of their neurodiverse family system is always more specific, more layered, and more particular than any framework can fully anticipate.
There is also a dimension of flexibility that is specific to Stage 3. Some clients will move through the ten steps entirely within Stages 1 and 2 and will never enter relational discussion, either because the conditions for it are not safe, or because the other parties in the system are not willing or prepared, or because the client's most important clinical work is individual clarity and the decisions that follow from it. That is not a partial use of the framework. As established in the previous section, individual integration is a complete and meaningful outcome in its own right, and a provider who treats it as incomplete because Stage 3 did not occur has misunderstood what the framework is designed to produce.
Other clients will move into Stage 3 at certain steps and not others, depending on what is ready, what is safe, and what the other parties in the system are prepared to engage with at any given point in the work. The relational discussion that is possible after Step 4, when clients have developed understanding of empathy differences, may look quite different from the relational discussion that becomes possible after Step 7, when clients have developed understanding of how trauma has shaped the system. Both are valid uses of Stage 3. Neither is more correct than the other. What matters is that the discussion happens after the individual integration it depends on, not before it.
What structure with flexibility ultimately looks like in practice is a provider who knows the framework well enough to hold it lightly, who can use the sequence as a guide without being governed by it, who can recognize when a client needs more time at a particular step and give it to them without anxiety about what is being delayed, and who can recognize when a client is ready to move forward and support that movement without rushing it. That kind of clinical judgment is not separable from the framework. It is what the framework is designed to develop in the providers who use it.
Section 5: Why This Approach Is Different From Traditional Family and Couples Work
Providers who encounter the R.E.A.L. Neurodiverse™ 10-Step Approach for the first time sometimes ask how it differs from existing family therapy or couples therapy models that have incorporated neurodiversity language. It is a fair question, and the answer matters, because the difference is not primarily one of terminology or cultural sensitivity. It is a difference in foundational assumptions about what neurodiverse family systems are, what they need, and what constitutes a successful outcome.
Most traditional family and couples therapy approaches share a set of assumptions that feel so reasonable they are rarely examined. The assumption that bringing people together into shared relational conversation is the natural and appropriate response to relational distress. The assumption that increased communication, when skillfully facilitated, moves toward understanding and repair. The assumption that the goal of the work is the preservation or restoration of the relationship in something close to its current form. The assumption that a provider who holds the space well enough can create conditions in which the system reorganizes itself toward greater health and connection (Kerr & Bowen, 1988).
These assumptions are not wrong in every context. In families and couples where neurological processing is broadly similar, where relational feedback lands in roughly compatible ways, where repair attempts are likely to be recognized and received as intended, they hold well enough to support effective work. But in neurodiverse family systems, where different neurologies create fundamentally different experiences of the same relational moment, where repair attempts frequently misfire not because of bad intent but because of neurological difference in how they are sent and received (Milton, 2012), and where the accumulation of those misfires has produced years of protective patterning, those assumptions fail in ways that can cause real harm.
The most common form that harm takes is not dramatic. It is the experience of having tried, again, in a structured therapeutic context, and arrived at the same place. One person explains and the other shuts down. One person seeks repair and the other experiences pressure. One person discloses pain and the other becomes defensive, not because they don't care, but because the relational dynamic the therapy was supposed to interrupt has simply found a new stage to perform on. The provider works hard. The family tries. And the session ends having rehearsed the pattern rather than interrupted it (Murgado-Willard, 2024).
The R.E.A.L. Neurodiverse™ Approach begins from different assumptions. It assumes that the family system is central but that bringing everyone into the same room is not always, or even usually, the right response to that centrality. It assumes that relational discussion is a tool with specific conditions of appropriate use, not a default setting for all relational work. It assumes that individual clarity is a complete and meaningful clinical outcome, not a consolation prize for clients who could not manage the relational work. And it assumes that the goal of the work is not repair or reconciliation in any predetermined form, but rather an honest understanding of what is actually possible in this particular system, given the neurological realities that are genuinely present and genuinely permanent.
This is also where the approach differs most significantly from models that have added neurodiversity language to existing frameworks without changing the underlying structure. Adding psychoeducation about autism to a couples therapy model does not change what the model assumes about how relational work should proceed. It does not change the assumption that communication skills will transfer from the session into daily life. It does not change the assumption that both partners are processing the session's relational content through compatible enough neurological pathways that the same intervention will land similarly for both of them. It does not address masking, or the gap between in-session presentation and daily life presentation (Hull et al., 2017), or the neurologically driven pull toward roles and cycles that reassert themselves the moment the session ends and the system's ordinary conditions resume.
The R.E.A.L. Neurodiverse™ Approach changes the structure, not just the language. It protects individual process before introducing relational complexity. It sequences the work around how understanding actually develops rather than around the assumption that understanding can be produced by putting people in a room together with a skilled facilitator. It holds consent and safety as non-negotiable conditions for relational discussion rather than as aspirations that the therapeutic relationship is assumed to have already established (Karakurt et al., 2016). And it treats neurological difference not as a complicating factor to be managed within an existing model, but as the central organizing reality of the system the work is designed to support.
For providers, this means that using the R.E.A.L. Neurodiverse™ Approach is not simply a matter of adding new content to existing practice. It requires a genuine reorientation of what the work is for, what success looks like, and what the provider's role is in relation to the system's own direction. That reorientation is not always easy. It asks providers to hold individual clarity as a sufficient outcome even when the presenting pain is relational and the pull toward joint intervention is strong. It asks them to treat the optionality of relational discussion as a clinical and ethical position rather than a structural concession. And it asks them to trust that a framework built around the neurological realities of the system will produce more durable outcomes than one built around assumptions that those realities quietly and persistently undermine.
Section 6: From Confusion to Clarity
The title of this post names a movement, and it is worth being precise about what that movement actually involves. Confusion to clarity is not a journey from not knowing to knowing, from distress to resolution, or from a broken family system to a repaired one. It is something more specific and more honest than any of those descriptions, and understanding what it actually is helps providers communicate the purpose of the work to clients in a way that sets accurate expectations from the beginning.
The confusion that neurodiverse family members carry is not simply a lack of information. It is a particular kind of disorientation that develops when a person has spent years, sometimes decades, trying to make sense of their relational experience using frameworks that were never adequate to explain it. They have tried harder, communicated more, accommodated more, set limits, sought therapy, read books, attended workshops, and still found themselves in the same place. The confusion is not the starting point. It is the accumulated residue of repeated attempts to solve a problem with tools that could not reach its actual source.
That kind of confusion has specific effects. It produces self-blame, because if the available explanations don't account for what is happening, the most available remaining explanation is that something is wrong with the person trying to make sense of it (Corden et al., 2021). It produces exhaustion, because navigating a system whose mechanisms are invisible requires an enormous and unsustainable amount of compensatory effort (Hull et al., 2017). It produces a particular kind of grief, the grief of not knowing whether the difficulty is real or perceived, whether the relationship is genuinely limited or whether better effort or better skill would finally produce the connection that has always felt just out of reach. And it produces, over time, a loss of trust in one's own perception, because the perception keeps pointing toward something that the available frameworks say should not be there.
Clarity, in the context of the R.E.A.L. Neurodiverse™ 10-Step Approach, is the restoration of accurate perception. It is what becomes possible when a client finally has a framework that matches what they have been experiencing. When the mechanisms that have been driving the family's patterns become visible and nameable. When the roles that felt like personality or pathology turn out to be neurologically rooted and systemically functional (Kerr & Bowen, 1988). When the cycles that felt random or deliberately cruel turn out to be predictable and mechanism-driven. When the grief that felt shameful or excessive turns out to be a completely reasonable response to a genuinely difficult situation that no one in the system had the tools to address.
Clarity is not the same as resolution. A client who reaches clarity about their neurodiverse family system may still be living inside significant difficulty. The neurological differences that shaped the system are still there. The accumulated history of misinterpretation is still there. The patterns that developed around neurological difference over years of daily life are still there, even when they are now understood. What clarity changes is not the terrain but the client's relationship to it. And that change in relationship, while it does not eliminate difficulty, transforms what the difficulty means and what the client can do in response to it.
From clarity, clients can make decisions that are grounded in reality rather than in confusion or hope. They can understand what is genuinely available for change and what is not, and stop spending energy on targets that the neurology of the system has always made unreachable. They can recognize their own role in the system's patterns without collapsing into blame, and take accountability for what is genuinely theirs without accepting responsibility for what was never theirs to carry. They can build limits that are realistic and connected to action rather than aspirational and dependent on the system's cooperation. They can grieve what has not been possible without treating that grief as evidence of personal failure (Corden et al., 2021). And they can make honest decisions about what level of contact, closeness, caregiving, and relational investment is sustainable given the system as it actually is.
For some clients, clarity leads toward relational discussion, toward the possibility of being seen accurately by the people they have been in relationship with, and of seeing them accurately in return. For others, clarity leads toward decisions about distance, separation, or the restructuring of contact in ways that are more honest about what the system can safely support. Neither of those outcomes is more successful than the other. Both are what clarity makes possible when it is genuine. And both are more durable than anything that could have been produced by moving toward relational discussion before the individual foundation was in place.
The R.E.A.L. Neurodiverse™ 10-Step Approach moves clients from confusion to clarity by giving them, at every step, the education they need to understand what has been happening, the individual integration space they need to make that understanding personally real, and the protection of knowing that relational discussion will only occur when it is safe, appropriate, and fully consented to by everyone involved. That sequence is not a detour from the work. It is the work. And for clients who have spent years trying to solve a neurologically rooted problem with tools that could not reach its source, it is often the first time the work has felt like it is finally aimed at the right thing.
Learn More
Providers who support neurodiverse families need a structured pathway that allows clients to build shared language, integrate insight individually, and only enter relational discussion when it is safe, appropriate, and fully consented to by all parties.
Continue to the Next Post: Why Providers Must Understand their Own Neurology
Works Cited
Bertilsdotter Rosqvist, H., Hultman, L., & Hallqvist, J. (2023). Knowing and accepting oneself: Exploring possibilities of self-awareness among working autistic young adults. Autism, 27(5), 1417–1425. https://doi.org/10.1177/13623613221137428
Corden, K., Brewer, R., & Cage, E. (2021). Personal identity after an autism diagnosis: Relationships with self-esteem, mental wellbeing, and diagnostic timing. Frontiers in Psychology, 12, Article 699335. https://doi.org/10.3389/fpsyg.2021.699335
Dziobek, I., Rogers, K., Fleck, S., Bahnemann, M., Heekeren, H. R., Wolf, O. T., & Convit, A. (2008). Dissociation of cognitive and emotional empathy in adults with Asperger syndrome using the Multifaceted Empathy Test (MET). Journal of Autism and Developmental Disorders, 38(3), 464–473. https://doi.org/10.1007/s10803-007-0486-x
Gallese, V. (2009). Mirror neurons, embodied simulation, and the neural basis of social identification. Psychoanalytic Dialogues, 19(5), 519–536. https://doi.org/10.1080/10481880903231910
Hull, L., Petrides, K. V., Allison, C., Smith, P., Baron-Cohen, S., Lai, M.-C., & Mandy, W. (2017). "Putting on my best normal": Social camouflaging in adults with autism spectrum conditions. Journal of Autism and Developmental Disorders, 47(8), 2519–2534. https://doi.org/10.1007/s10803-017-3166-5
Karakurt, G., Whiting, K., van Esch, C., Bolen, S. D., & Calabrese, J. R. (2016). Couples therapy for intimate partner violence: A systematic review and meta-analysis. Journal of Marital and Family Therapy, 42(4), 567–583. https://doi.org/10.1111/jmft.12178
Kassing, K., & Collins, A. (2026). “Slowly, over time, you completely lose yourself”: Conceptualizing coercive control trauma in intimate partner relationships. Journal of Interpersonal Violence, 41(3–4), 662–684. https://doi.org/10.1177/08862605251320998
Kerr, M. E., & Bowen, M. (1988). Family evaluation: An approach based on Bowen theory. W. W. Norton & Company.
Mahler, K., Hample, K., Jones, C., Sensenig, J., Thomasco, P., & Hilton, C. (2022). Impact of an interoception-based program on emotion regulation in autistic children. Occupational Therapy International, 2022, Article 9328967. https://doi.org/10.1155/2022/9328967
Milton, D. E. M. (2012). On the ontological status of autism: The 'double empathy problem.' Disability & Society, 27(6), 883–887. https://doi.org/10.1080/09687599.2012.710008
Murgado-Willard, K. (2024). Neurodiverse couple therapy: A practical guide to brain-informed care. Routledge. https://doi.org/10.4324/9781003351337
Oehme, K., Bradley, L., Cameron, M., Perko, A., & Clark, J. (2024). Increasing multidisciplinary professionals’ capacity to support neurodiverse families. Diversity & Inclusion Research, 1(1), Article e12003. https://doi.org/10.1002/dvr2.12003
Shaw, P., Stringaris, A., Nigg, J., & Leibenluft, E. (2014). Emotion dysregulation in attention deficit hyperactivity disorder. American Journal of Psychiatry, 171(3), 276–293. https://doi.org/10.1176/appi.ajp.2013.13070966
van der Kolk, B. A. (2014). The body keeps the score: Brain, mind, and body in the healing of trauma. Viking.

© 2023 REAL Neurodiverse
All Rights Reserved
anne@neurodiversemarriage.com
Text or Call: (617) 996-7239 (United States)